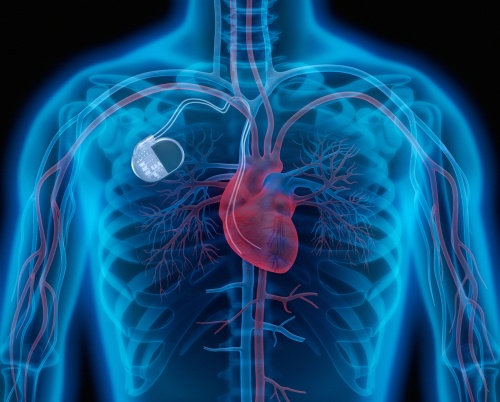
Implantable cardiac monitoring (ICM) to look for arrhythmias in post MI patients and prompt treatment did not provide clinical benefit, according to the results of the BIO-GUARD|MI trial. Interestingly though, ICM in higher risk Non-ST Elevation Myocardial Infarction (NSTEMI) patients appeared to have clinical benefits according to the study authors.
The trial was stopped early to resolve bias due to inconsistent reporting of non-cardiovascular events in the control group. This resulted in lower-than-expected primary endpoint events which consequently decreased the power of the study.
The BIO-GUARD|MI trial included a total of 790 patients, in the highest risk population post myocardial infarction defined by a high CHADS-VASC score (average of 4.8), from 60 medical centers in Europe, Australia and the United States. Half the patients were randomized to undergo implantable continuous monitoring. There was no reduction of primary endpoint at 2 years, defined by cardiovascular mortality or hospitalization for arrhythmia, acute coronary syndrome, worsening of heart failure, stroke, systemic embolism, and major bleeding.
However, predefined subgroup analysis based on type of MI (STEMI vs nSTEMI) showed reduction of primary endpoint in NSTEMI patients by 30%. This group of high-risk patients were expected to benefit the most from intense arrhythmia monitoring in the form of implantable cardiac monitoring in the post MI setting.
“The trial showed responding to short lasting asymptotic arrhythmias can improve outcome if done in a population of high enough risk” said Dr. Christian Jons, lead author of the trial (Electrophysiologist at the Department of Cardiology at Rigshospitalet Copenhagen in Denmark).
The available data analysis from this trial is intriguing as it showed some advantages from implantable devices monitoring and treatment of patients with no symptoms or low burden symptoms in NSTEMI population. When Dr. Jons was asked about possible replication of this trial, he said “800 patients randomized with loop recorder over 7 years is a very long time, I think we will not see a trial in the next couple of years like this one, … However, the future is coming up with s sort of devices that can measure body function”.
As wearable technology and the ability to monitor arrythmias becomes more ubiquitous the medical community continues to grapple and understand how to leverage these devices to improve patient outcomes. Investigators of future studies may elect to focus on post nSTEMI high risk patient populations to further understand and evaluate the benefit of these technologies in these settings.
@KahtanAlfadhl discusses the BIOGUARD-MI trial with Dr. Jons at #ACC22. #FITsOnTheGo #ACC22 #ACCFIT #ACCEarlyCareer #MedTwitter @MayoCVFellows @DanDaviesMD @VinayakKumarMD @ACCinTouch @TTUHSC pic.twitter.com/vhKjfj2fa3
— FITsOnTheGo (@FITsOnTheGo) April 4, 2022
Fill video link:
BIOGUARD-MI with Dr. Christian Jons
References:
Jons C. The clinical effect of arrhythmia monitoring after myocardial infarction (BIO-GUARD|MI) Presented at the ACC.22 World Congress of Cardiology; April 4, Washington, D.C.


 © 2025 Mashup Media, LLC, a Formedics Property. All Rights Reserved.
© 2025 Mashup Media, LLC, a Formedics Property. All Rights Reserved.