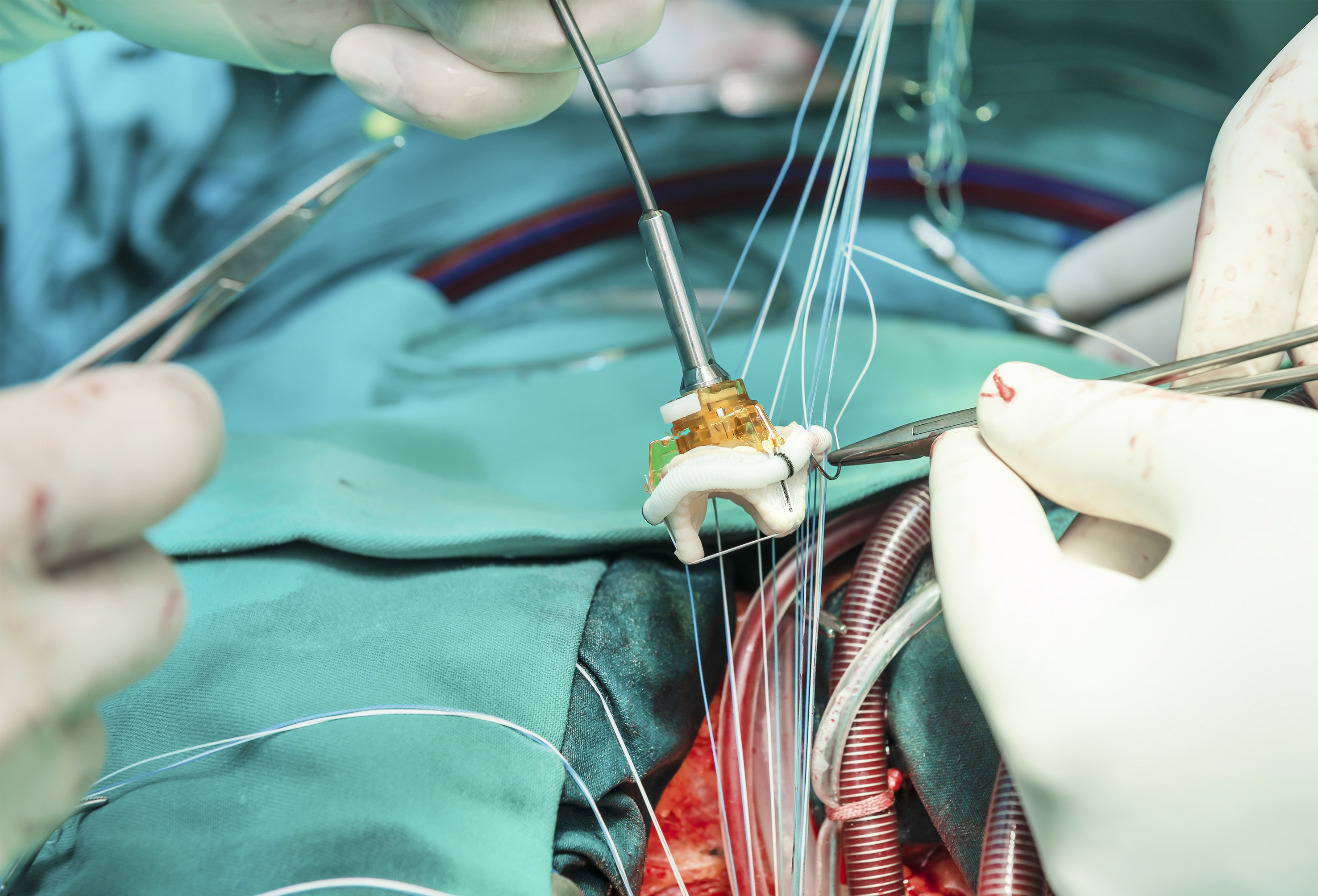
The use of transcatheter aortic valve replacement (TAVR) with a novel self-expanding aortic valve was shown to be noninferior to surgical aortic valve replacement (SAVR), new study results presented at the American College of Cardiology Annual Scientific Session in New Orleans suggested.
Researchers for the Evolut Low Risk noninferiority trial, seeking to assess the safety and efficacy of TAVR with the Evolut self-expanding supra-annular valve compared to surgical aortic valve replacement in patients with a low predicted risk for 30-day surgical mortality randomly assigned (1:1) patients to undergo either TAVR (n=725) or SAVR (n=678). The primary study endpoint was a composite of all-cause mortality or disabling stroke at two years. Mean patient age was 74 years.
According to the study results, TAVR was shown to be noninferior to SAVR for the primary endpoint (5.3% TAVR vs. 6.7% SAVR; absolute difference, -1.4% (95% CI, -4.9 to 2.1). The researchers also reported that all hierarchical secondary endpoints were met as well. The researchers also reported that for estimated Kaplan-Meier rates of death, disabling stroke and heart failure hospitalizations at one year, TAVR was superior to SAVR (5.6% vs. 10.2%, P=0.002 for difference), and that TAVR patients tended to have shorter procedural times and lengths of stay compared to SAVR. Patients in the TAVR group also had lower aortic valve gradients (8.6 mm Hg vs. 11.2 mm Hg) compared to SAVR patients and larger effective orifice areas (2.3cm2 vs. 2.0 cm2).
As Good As Surgery
“TAVR with self-expanding supra-annular valves was noninferior to surgery in patients with severe aortic stenosis at low surgical risk,” lead study author Michael J. Reardon, MD, professor and Allison Family Distinguished Chair of Cardiovascular Research at Houston Methodist Hospital and the study’s senior author, said in his presentation. “At 30 days, TAVR showed far better safety and recovery profile than surgery, with less death or disabling stroke, less disabling stroke, shorter length of stay, and better quality of life while surgical valve replacement had fewer pacemakers implanted and less residual aortic regurgitation.”
He went on to suggest that TAVR maybe be the optimal path in this population.
“We now have a minimally invasive procedure that is as good as or better than surgery, while at the same time allowing most patients to be out of the hospital within a few days and be back to their normal activities within a week, and that’s pretty important,” said Dr. Reardon in an accompanying press release. “We’ve now looked at a broad risk spectrum of patients—those at high, intermediate and low surgical risk—and these series of trials have shown that TAVR is better than or as good as surgery in terms of disabling strokes and deaths from all causes. Given this data, it now seems reasonable to consider moving TAVR in low risk patients to a class I guideline indication on par with surgery for patients with severe aortic stenosis.”
The full manuscript was published simultaneously in the New England Journal of Medicine.




 © 2025 Mashup Media, LLC, a Formedics Property. All Rights Reserved.
© 2025 Mashup Media, LLC, a Formedics Property. All Rights Reserved.