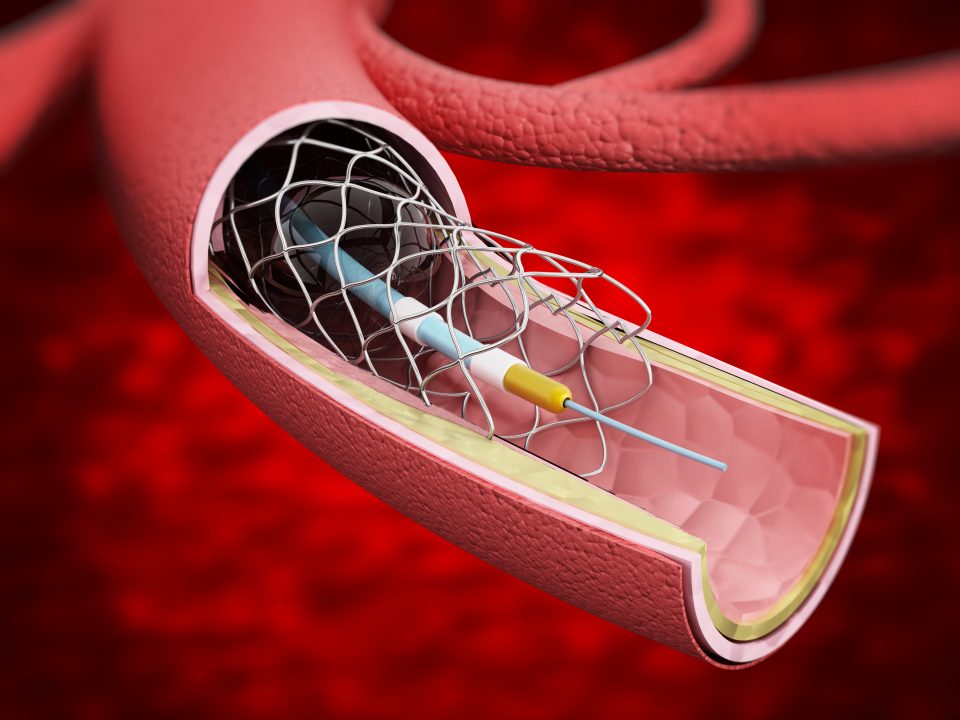
New research presented at Transcatheter Cardiovascular Therapeutics (TCT) 2020 showed that coronary intravascular lithotripsy (IVL) safely and effectively enabled stent delivery in severely calcified lesions.
Stent under expansion caused by coronary calcification is a significant predictor of subsequent stent thrombosis and restenosis. IVL technology emits circumferential pulsatile energy to modify calcified plaque, which can augment stent implantation. The Disrupt CAD III trial aimed to determine the safety and effectiveness of coronary IVL to optimize stent deployment in de novo stenoses involving severely calcified vessels. The non-controlled, single-arm multicenter trial was designed for U.S. regulatory approval of this technology as an addendum to coronary stenting.
The authors enrolled 384 patients with stable, unstable, or silent ischemia and severely calcified de novo coronary artery lesions undergoing percutaneous coronary intervention (PCI). Target lesions were fitted with IVL catheters and received 10 IVL pulses followed by temporary IVL balloon inflation. Treatment was repeated until full balloon expansion was achieved, with a maximum number of 80 pulses. If maximum pulses were delivered but lesion preparation remained incomplete (i.e., residual stenosis >50%), an additional IVL catheter could be implemented. Post-procedure assessments were required within 12-24 hours, and follow-up was conducted after 30 days and at 6, 12, and 24 months
The study’s primary safety and efficacy endpoints, respectively, were freedom from Major Adverse Cardiovascular Events (MACE) at 30 days and successful stent implantation with less than 50% residual stenosis and were compared to a pre-specified performance goal. An optical coherence tomography (OCT) sub-study was performed to assess calcium modification.
Primary safety and effectiveness endpoints were achieved in 92.2% and 92.4% of patients, respectively (P<0.0001). Perforation, abrupt closure, and no-flow were not observed post-IVL prior to stent placement. OCT found multi-plane and longitudinal calcium fractures after IVL in 67.4% of lesions. Minimum stent area was 6.5 ± 2.1mm2 and was similar regardless of demonstrable fractures.
Overall, IVL prior to stent implantation was well tolerated with low rates of major peri-procedural clinical and angiographic complications.
#TCT2020 Late-Breaking Science: The Disrupt CAD III Study demonstrated safety and efficacy of intravascular lithotripsy to optimize stent expansion in severely calcified #cvCAD. Read in #JACC. https://t.co/XH2zEyGCrm@DrJMHill @djkereiakes @drdrewkleinphi @GreggWStone pic.twitter.com/KTP2zPy3wb
— JACC Journals (@JACCJournals) October 15, 2020
@djkereiakes DISRUPT CAD III achieves both primary safety & efficacy endpoints for #coronary #IVL for severe calcific lesions by multiplane and longitudinal calcium fracture#TCT2020 #TCTConnect @crfheart @ziadalinyc @Drroxmehran @SukhNijjer @nolanjimradial @ncurzen @ShrillaB pic.twitter.com/iki30OnBo3
— Aaysha Cader (@aayshacader) October 15, 2020



 © 2025 Mashup Media, LLC, a Formedics Property. All Rights Reserved.
© 2025 Mashup Media, LLC, a Formedics Property. All Rights Reserved.